Getting to know what Bipolar Disorder is: what are the types and criteria for diagnosis? What are the five main myths about it?

Summary of contents
- What is Bipolar Disorder?
- What is a depressive episode? What is a manic episode?
- Is that all there is? Are there other types?
- What are the types of Bipolar Disorder?
- Is there a treatment?
- What are the 5 myths around Bipolar Disorders?
What is Bipolar Disorder?
The word "bipolar" has become a part of everyday conversation. It's often used to describe a person who has mood swings or is in between two options to decide. Bipolar disorder is much more than that.
When we talk about Bipolar Disorder, we refer to a chronic mental illness that affects a human's emotional part. It is a mood disorder in which patients may experience bad and very good mood periods. The period of good mood is known as the "manic episode," and the period of a bad mood is known as the "depressive episode." These episodes are alternating and opposed, hence the name of Bipolar Disorder".
Between these episodes, the patient's mood may return to normal levels; however, even in conditions of normalcy, the disorder significantly burdens people with bipolar disorder and those around them, as it causes functional impairment in many areas of their daily lives.
What is a depressive episode? What is a manic episode?
Depressive episodes
Although a major depressive episode is not a prerequisite for diagnosing bipolar disorder, these types of episodes often alternate with manic episodes. Persistent and constant sadness occurs more often than rage in many people with bipolar disorder. Depressive episodes are a serious medical condition that negatively affects the way a depressed patient feels, thinks, and acts.

Five (or more) of the following symptoms occur in patients for at least two weeks and represent a change in previous functionality. At least one of the symptoms has to be: 1) depressed mood, or 2) loss of interest or pleasure. The following symptoms can be reported by observation and recording of others.
- Severe decrease in interest or pleasure in all or almost all activities for most of the day
- Significant weight loss (while not on a diet), weight gain, or decreased or increased appetite. Children: failure to absorb the expected weight
- Insomnia or hypersomnia
- Fatigue or loss of energy
- Feelings of worthlessness or excessive or inappropriate guilt (which can be delusional), not just self-loathing or guilt because you are sick
- Decreased ability to think or concentrate or indecision (by subjective assessment or observation)
- Repeated thoughts of death (not just fear of death), recurrent suicidal ideation, without a specific plan or suicide attempt or a specific plan to commit suicide
Manic episodes
The manic phase of bipolar disorder involves unusually high energy and activity level. It is a distinct pathologically and persistently increased, diffuse or irritable mood. To consider the possibility of bipolar disorder, the person must have at least one manic episode. During manic episodes, people may exhibit daring, aggressive, or bizarre behavior that they did not previously have. The symptoms are not due to the actions of a substance or a general physical condition.

Three or more of the following symptoms should occur in patients (4 if the mood is only irritable) and should last at least a week.
- Swollen self-esteem or a sense of grandeur
- Reduced need for sleep
- More talkativeness than usual or pressure to keep talking
- Loss of ideas or subjective feeling that thoughts are galloping
- Distraction
- Increase of targeted activity and speech
- Excessive involvement in enjoyable activities that have a high probability of painful consequences
- The symptoms do not meet the criteria of a mixed episode
- Severe reduction in functionality or social activities or relationships with others, or hospitalization is necessary, or there are psychotic elements
Is that all there is? Are there other types?
In addition to the depressive and manic episodes, there are two other types of episodes that one can encounter in bipolar disorder.
Hypomania
A hypomanic episode has similar symptoms to a manic episode. It is the state of hyperactivity of the brain and body but with less clinical representation.
It lasts for at least four days, with symptoms of the episode appearing most of the day and almost every day. In general, a hypomanic episode does not cause as many serious problems at work or in a person's personal life as a manic episode.
These episodes are perhaps the most difficult to diagnose, as the patient is functional and overproductive for long periods without reaching the levels of intensity and severity of mania.

- Ιnflated self-esteem or a sense of grandeur
- Reduced need for sleep (e.g., the person feels rested after only 3 hours of sleep)
- More talkativeness than usual or pressure to keep talking
- Flight of ideas or subjective feeling that thoughts are galloping distraction (attention is easily distracted by trivial or irrelevant external stimuli)
- Increase in targeted activity; the person is overactive (either socially, at work or school, or sexually)
- Excessive engagement in enjoyable activities that have a high probability of painful consequences (e.g., the person engages in unrestricted indiscriminate shopping, sexual discrimination, or foolish business investments)
Mixed episodes
More rarely, some patients show mixed symptoms. Mixed episodes are characterized by depressive, hypomanic, manic symptoms, or rapid alternation of the three types of symptoms. Thus, they could look depressed or have some signs of depression but have increased sexual appetite, galloping thoughts, or spend excessive amounts on products they would not buy.
What are the types of Bipolar Disorder?
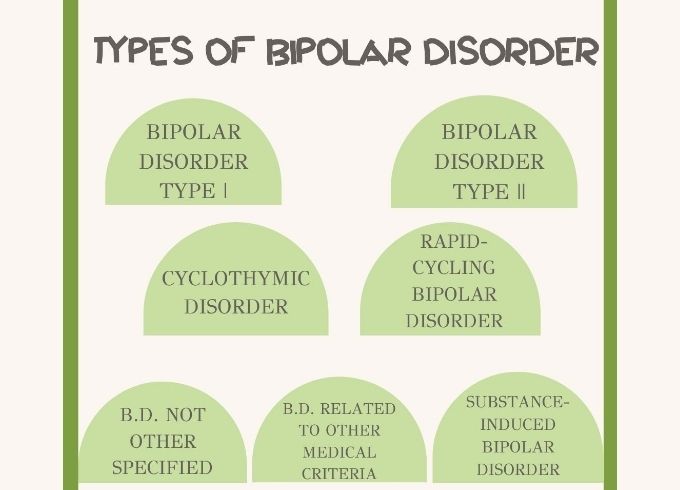
Bipolar Disorder consists of the following types:
Bipolar Disorder Type I
To be diagnosed with bipolar I disorder, a person must meet the full criteria for a manic episode, which includes three of the following symptoms:
- Increased speech
- Increased self-esteem or grandeur
- Reduced need for sleep
- Increased energy, goal-oriented activities, or irritability
- Competitive thoughts
- Reduced attention span
- Increased risk-taking behavior
Manic episodes of bipolar disorder are preceded or followed by a major depressive episode. The depressive episode lasts for at least two weeks. Episodes of mania or mixed episodes (mania-depression) lasting at least seven days or severe episodes of mania requiring admission to a hospital or clinic. There are also episodes of depression, which usually last two weeks or more.
Frequency: 0.3%-1.5% of the population
Bipolar disorder type II
This type is characterized by a combination of depressive episodes and mild mania, with no severe flare-ups or mixed episodes.
A person can be diagnosed with bipolar II disorder if they have had an episode of hypomania, along with a depressive episode characterized by at least five of the following symptoms:
- Depressed mood
- Changes in sleep patterns
- Changes in dietary patterns
- Lack of energy or fatigue
- Loss of interest and pleasure in the activities he had previously enjoyed
- Feeling anxious or slow
- Feelings of guilt or non-existence
- Difficulty concentrating or making decisions
- Suicidal thoughts
Frequency 0.4% - 5% of the population
Cyclothymic Disorder
An extremely mild form of bipolar disorder. People with the cyclothymic disorder(or mood-swings disorder) have episodes of hypomania and mild episodes of depression for at least two years. While daily life can be difficult for people suffering from mood disorders, the condition usually does not affect daily functioning, although it can be chronic and worsen over time. However, the symptoms do not fall under any of the above definitions of bipolar disorder.
Compared to the diagnosis of bipolar I and bipolar II disorders, which are somewhat straightforward when it comes to warning symptoms, mood-swings disorder is often more challenging to diagnose. Patients should experience the following diagnostic symptoms:
- Many periods of hypomanic symptoms for at least two years that do not meet the criteria for hypomanic episodes
- Many periods of depressive symptoms do not meet the criteria for a major depressive episode
- The person has experienced these periods for at least half of the time, and the person has not had symptoms for more than two months.
Frequency: 1% of the population

Rapid-Cycling Bipolar Disorder
This is a more complicated version of bipolar disorder. In this case, there are four or more episodes of major depression, mania, hypomania, or mixed episodes over a year. Women may be more likely to have bipolar disorder, and also, it is more common in people whose first episode occurred when they were young.
Bipolar Disorder Not Other Specified
The typical symptoms of bipolar disorder are present, but the symptoms do not meet the criteria for any of the above disorders. In any case, the individual's behavior does not fall into the usual (expected) standards. Clinicians sometimes diagnose patients with major depression instead of bipolar II disorder if they do not disclose information about their hypomanic episodes.
Bipolar disorder not classified elsewhere is often diagnosed in patients with brief episodes of depression and hypomania that are not classified as mood disorders. Diagnostic criteria may also include multiple episodes of hypomania with or without depressive episodes.
Bipolar disorder related to other medical criteria
A psychotherapist can diagnose a patient with a bipolar disorder associated with another medical condition if symptoms have a co-occurring medical condition. Symptoms may be short-lived or may continue after the condition has subsided.

Some medical conditions cause changes in the brain that can lead to mental health conditions. Brain tumors, traumatic brain injury, multiple sclerosis, migraines, and strokes are some examples of physical conditions that can change brain function.
Substance-Induced Bipolar Disorder
A person can be diagnosed with substance-induced bipolar disorder if they experience symptoms while taking or withdrawing a drug or other substance. Many different drugs and substances have been linked to substance-induced bipolar disorder. In addition to substance-induced bipolar disorder, medications, other substances, or withdrawal from these substances may cause other substance-induced disorders, including anxiety disorders, depression, obsessive-compulsive disorder, and neurological disorders.
Is there a treatment?
The treatment of Bipolar Disorder is based on the types and severity of symptoms that a person may experience and has to be highly individualized. The treatment is suggested to be a combination of medication and psychotherapy, the most effective treatment.
The medication used is as follows:
- Stabilizers
to stabilize mood swings
- Antipsychotic
to control psychotic symptoms such as delusions, hallucinations, and severe manic traits
- Antidepressants
less commonly prescribed, as they can cause a manic episode
The psychotherapeutic approach that will be applied depends on the course of the disorder, the phase of the patient (manic-hypomanic-depressive episode), the individual's history, the medication the client receives, and their cognitive abilities.
The most common treatments are:
Cognitive Behavioral Therapy would be helpful for clients to recognize their depressive thoughts and behaviors and alternate them. It helps significantly reduce the intensity of persistent psychotic symptoms, which leads to fewer episodes of relapse.
Family psychotherapy would be beneficial, where a helping hand for stress reduction is also given to the family of a person with bipolar disorder. Next, people with the condition need to have a support network that understands their needs and learns the theoretical background of the disease and its subsequent management.
Psychosocial interventions refer to the supportive techniques that aim to integrate the person with a mental disorder in society, socialize with other members, and have opportunities for personal development as a citizen and social being. Such can be Supported Employment, for example, an approach that ensures a job to people with mental illnesses, or Training in Social Skills where patients are taught skills that help them in their interpersonal relationships, such as starting a conversation or expressing how they feel.

Although the prevalence of the disorder is small, it is widespread in conversations between people, where everyone gives their version of the characteristics of the disorder without knowing precisely what it is about. This has led to the oversimplification of the disorder, misinformation around bipolar disorder, and different ideas about what ultimately turn out to be myth.
What are the 5 myths around Bipolar Disorders?
1. Being bipolar as just changing mind and mood
Many people are in a hurry to characterize a person as bipolar when it is simply difficult to decide and come to a decision and jump from one to the other. For example, you can easily find someone being bipolar when they can review and do another opposite from one food choice in a restaurant (e.g., from something spicy to something mild & sweet). People often associate it with extreme mood changes, even if it concerns moods beyond depression and mania. An example could be if someone is being enthusiastic about a party they are going to meet his friends and then when the day and time is approaching, they get bored and cancel the party.

These mood swings, which are common to all of us at times, do not last a few minutes, but can last from weeks to months, making the situation more severe and utterly irrelevant to the simple case of mood swings. Bipolar disorder is much more than that change. And of course, the content, duration, and frequency of these changes are of major importance for diagnosing the disorder. This myth has focused on one essential element of the disorder and has given it a different extension.
2. There is no cure- it's just genetics
Another myth that prevails out there is that bipolar disorder is not curable and that the absolute genetic origin stigmatizes you forever. The truth is that research has shown that people who have a close relative with bipolar disorder are more likely to develop the disorder themselves. It has been found that combining abnormalities in many genes increases the risk of developing the disorder, but the exact way this occurs remains unclear.
The genetic predisposition to the disorder is not enough to cause it to manifest on its own. Environmental factors necessarily trigger the onset of the disorder in individuals carrying the relevant gene variants. This fact proves that this is a disorder with a lot of room for improvement, and depending on the case, treatment is possible. As we have seen above, many therapeutic approaches can bring about significant changes in the individual and the person's life with the disorder.
3. Sufferers are violent
One belief that is an apparent myth for people with bipolar disorder is violent and dangerous. It is difficult to justify such a connection, and above all, a disorder alone is not enough to explain aggressive behavior. There are always more factors that can affect mood and lead to aggressive behaviors such as increased stress or substance and alcohol abuse.
Bearing in mind that environmental factors also play a role in the development of the disorder, it is difficult to judge that the disorder may be responsible for some manifestation of aggression. The absence of a supportive social network, child trauma, and sociocultural factors, can be examples of the influence of the environment on aggressive behavior.
Given the symptoms of depressive and manic episodes in bipolar disorder, it is more likely that the person will behave aggressively and put themselves in danger rather than doing something similar to others.
4. Only adults can develop it
It is heard in everyday life that bipolar disorder is a disorder that affects only the adult world. That one can not manifest these symptoms before adulthood and that it is a serious disorder that is impossible to hurt children. Bipolar disorder can occur during adolescence or even in childhood. As would be expected, the risk is greater for children whose parents have bipolar disorder.
Unlike adults, who experience distinct periods of mania or depression, children and adolescents usually experience rapid mood swings, even over a day. In phases of mania, a child becomes supple, destructive, and has many outbursts. In contrast, in phases of depression the symptoms take a more organic form and are experienced as a headache or stomachache.
The disorder usually presents with mixed symptoms in adolescents, while the signs in older adolescents are similar to those of adults. However, it is more challenging to diagnose young people. There are several times where there's a misdiagnosis is given, and children with bipolar disorder are diagnosed with depression or Attention Deficit Hyperactivity Disorder.
5. Mania means productivity
One last myth commonly reproduced for people with bipolar disorder is that the period of mania can be very productive. This myth is based on the increased energy levels that prevail during the onset of the manic episode. Most people believe that the increased self-esteem and sense of greatness that people with bipolar disorder can feel makes them capable of responding to any situation.

Realistically, what happens does not have such a healthy-productive ending. A person with bipolar disorder can make bad moves or put themselves in danger; for example, he can spend vast sums of money during a manic episode or follow unsafe and dangerous practices in sexual intercourse. The results of such acts can be irreparable and undesirable for the person when the period of mania is over.
It is important to consult a mental health professional if you feel that you or a person from your social environment is related to something of the above in order to receive timely treatment and ensure a better and more qualitative life.
Get to know us more!
If you would like to get involved in this initiative and be a part of history in the making, feel free to shoot us an email at contact@buddyhelp.org, or browse our website to discover all of the many ways you can join our BuddyHelp family and make a difference in the world.
